The story in four numbers
Anya saw a problem the world had accepted. She decided not to.
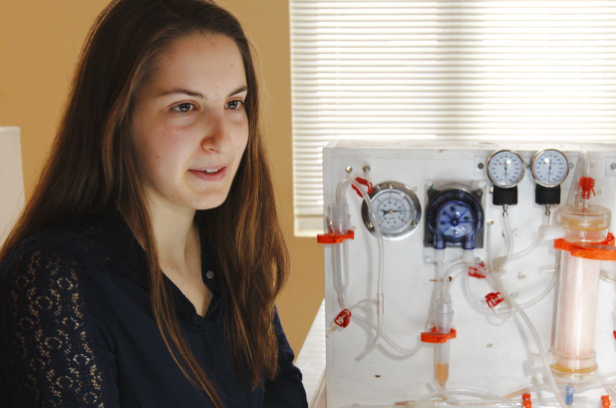
Most people, when they learn that a life-saving medical treatment is priced beyond the reach of millions, accept it as an unfortunate fact about how the world works. Anya Pogharian decided, instead, to build a solution in her kitchen. The result — a prototype she calls HemoAccess — is a fully functional dialysis machine capable of filtering blood for kidney-failure patients, assembled from off-the-shelf components and open-source software, for roughly the price of a mid-range smartphone.
The breakthrough here is not the science of dialysis — that has existed for decades. The breakthrough is the price, and the design philosophy that produced it. Pogharian did not start from a hospital specification and try to cut cost. She started from the patient who has no machine at all, and built the smallest viable thing that would save them. That inversion — from clinical-grade-minus to patient-grade-plus — is what frugal engineering at its best actually looks like.
Anya Pogharian did not discover dialysis. She discovered that dialysis does not have to cost what it costs — and then she proved it. Those are two very different kinds of genius, and the second one may be the rarer of the two.
The machine itself — what she built and how it works
Understanding the engineering matters, because the device is not a science-fair curiosity. It is a functional medical prototype with a deployment thesis. The machine does not try to replicate what hospital dialysis equipment does. It identifies what a kidney-failure patient in a remote clinic actually needs and delivers exactly that, nothing more.
| Attribute | Specification | Why it matters |
|---|---|---|
| Form factor | Tabletop portable | Compact enough for rural clinics, mobile units, refugee-camp medical stations, post-disaster deployments |
| Estimated build cost | < $1,000 | Off-the-shelf globally available components; fraction of the $20K–$80K cost of hospital-grade machines |
| Core process | Two-pass filtration | Blood drawn through a semipermeable membrane against a dialysate solution; waste removed by diffusion; clean blood returned |
| Safety system | Automated sensors | Pressure and flow monitored continuously; pump auto-adjusts to stay inside safe parameters; alerts for circuit irregularities |
| Power requirement | Low — generator-viable | Operates on portable power stations and backup generators; viable in settings with unreliable grid electricity |
| Software | Open-source | Control software fully open-source; any engineer worldwide can modify, improve, or adapt without licensing friction |
| Component sourcing | Global availability | Every component deliberately selected so no proprietary part depends on a single supplier |
| Maintenance | Field-repairable | Designed for maintainability in low-resource settings; no specialist technician required for standard part replacement |
The design insight is profound in its simplicity. Hospital dialysis machines are built to serve multiple patients per shift inside a clinical environment with trained staff, reliable infrastructure, and specialist maintenance. They integrate extensive redundancy because the environment demands it — and because the market that buys them can absorb the cost. Her machine asks a different question: what does a single patient in a remote clinic, served by a community health worker with basic training, actually need to receive life-sustaining dialysis? The answer is: a reliable pump, a clean filter, a sensor that catches dangerous pressure changes, and a control system simple enough to operate without specialist knowledge. Everything else — every additional subsystem, every redundant module, every clinical-grade interface — is a feature that serves the hospital, not the patient.
The machine she did not build is as important as the one she did. Every component she chose to leave out was a deliberate act of engineering empathy — asking who will use this, where, and with what resources, and designing for that reality.
The people she built it for — the scale of the gap
The motivation behind the invention was not abstract. The gap between the people who need dialysis and the people who can access it is one of the starkest healthcare inequities on the planet — and it is driven by price, not by the absence of medical knowledge.
A mobile health NGO that currently cannot carry dialysis equipment into a disaster zone could carry several of her units in a single van. International medical teams in refugee camps have already requested testing units. Humanitarian organisations working in Africa, South Asia, and South America have begun evaluating the device for field deployment. The interest is not theoretical — it is operational.
Pogharian is not alone — a lineage of young inventors
History has a long record of young people — unbound by the professional assumptions and institutional constraints that accumulate with experience — solving problems their elders had learned to accept. Anya Pogharian joins that lineage. The pattern is consistent enough to be its own category of innovation.
| Age | Inventor | What they built | Year |
|---|---|---|---|
| 14 | Philo Farnsworth | Conceived the basic design for electronic television — sketched on a chalkboard for his chemistry teacher | Idaho, 1920 |
| 15 | Louis Braille | Invented the tactile reading system used by blind people worldwide — and published a complete working version | Paris, 1824 |
| 15 | Ann Makosinski | Built a flashlight powered by body heat — won Google Science Fair global prize; no batteries, just human warmth | Canada, 2013 |
| — | Anya Pogharian | Built a fully functional portable dialysis machine — HemoAccess — for roughly the price of a smartphone, using off-the-shelf parts and open-source software; aimed at low-resource clinics | Canada, 2025 |
The pattern is consistent: the teenage inventor succeeds not in spite of their inexperience but partly because of it. Professional engineers in established fields accumulate not only expertise but also assumptions — about how complex a solution needs to be, how much it should cost, what trade-offs are acceptable. Young inventors, coming to a problem fresh, sometimes ask questions experience has trained professionals not to ask.
Professional medical-device engineers know an enormous amount that she does not: regulatory pathways, clinical validation, manufacturing tolerances, sterilisation protocols, long-term material performance. That expertise will be essential in taking her prototype from kitchen to clinic. But those same engineers had largely accepted that a low-cost field dialysis machine was not commercially viable. She had the advantage of not knowing that — and therefore not being stopped by it.
By building on open-source designs and releasing her own work under an open licence, she ensures that her breakthrough belongs to everyone. Engineers anywhere can take her design, improve it, adapt it for local conditions, manufacture it locally. This is not a product — it is a platform. The multiplier of open-source innovation means a single invention can spawn hundreds of regional variants, each tuned to its own clinic, climate, and supply chain.
From prototype to the world — the road ahead
The journey between a remarkable kitchen prototype and a device deployed in thousands of clinics across three continents is real, and it is not short. Clinical validation, regulatory certification, and manufacturing scale-up are processes measured in years. But they are not impossible — and she does not have to navigate them alone.
| Stage | What happens | Who can help |
|---|---|---|
| Design partnership | Engineers refine the prototype for durability, consistency, and field reliability under real-world stress | University biomedical engineering departments, humanitarian tech labs |
| Clinical safety testing | Controlled trials with medical-ethics approval to demonstrate safety and efficacy for human use | Hospital research departments, global health institutions |
| NGO pilot deployment | Partnerships with MSF, Partners in Health, or equivalent — real-world low-resource clinical settings, collected operational data | NGOs already expressing interest; international emergency medical teams |
| Regulatory certification | WHO pre-qualification or national regulatory approval in target deployment countries | Development finance institutions, global health foundations |
| Manufacturing at scale | Distributed or local manufacturing in high-need regions — leveraging the open-source design to enable local production without IP barriers | Social-enterprise manufacturers, DFI financing, impact investors |
The open-source architecture of her design means that its impact is not contingent on any single path to scale. Engineers in Nigeria, India, and Bangladesh who read her design and build their own variants adapted to local conditions may ultimately reach more patients than any single centralised manufacturing effort. The invention does not need to scale through one channel — it can scale through all of them simultaneously.
Age is not a precondition for changing the world
There is a version of this story that could be told as a celebration of an exceptional individual — a gifted teenager who did something most people could not do. That version is true, but it is incomplete. The more important message of what Anya Pogharian achieved is not about her exceptional qualities. It is about what becomes possible when someone refuses to accept the limits of what already exists.
She did not have access to a laboratory. She did not have a research budget, a team of engineers, or decades of professional experience. She had a kitchen table, off-the-shelf components, open-source software, and the conviction that a problem as consequential as kidney-failure mortality in low-income countries deserved a better answer than the one the market had provided.
For those of us who work in investment, strategy, and innovation, her achievement is also a reminder of something institutional life can cause us to forget: the most important breakthroughs are not always the most expensive ones. Sometimes the breakthrough is a question asked from a fresh perspective — and the determination to keep asking it until the answer becomes a machine that can save a million lives.
Anya Pogharian was a teenager when she built a dialysis machine in her kitchen. She designed it for people she will likely never meet, in communities she may never visit, with a compassion most adults — with all their resources and experience — somehow never found time to act on. That is not just inspiring. It is instructive.
Sources: Public coverage of Anya Pogharian and the HemoAccess prototype · ISN Global Kidney Health Atlas (2023) · Lancet Global Health (Bello et al., 2024) · PMC publications on global kidney replacement therapy access.